|
I have been searching for any peer reviewed data which suggests 25 mcg should be regarded as an upper limit of vitamin D supplementation and in my search I have found this page https://www.nrv.gov.au/nutrients/vitamin-d which seems to be a joint effort by Ministry of Health New Zealand and the Australian authority and which suggests an upper limit of 80 mcg per day with an 'uncertainty level' of 1.2 and a 'no observed adverse effect level' of 100 mcg.
Would you please let me know what peer reviewed literature the current limits of 25 mcg were based on? I have personally been researching a number of avenues in regards to the health of my wife and myself over the last 5 years. Coming out of winter in 2015 I decided to measure my 25(OH)D levels and found them at 61 nmol/L in the range 50-150. My research indicated that this was less than what I wanted but nevertheless established a baseline for my own experimentation. I began supplementing at 5000IU daily with the product I obtained through iHerb and which most recently you have seized at the border. There are many potential benefits of having high serum levels of 25(OH)D and it appears that the NZ Ministry of Health only focuses on the potential for decreasing risk of osteoporosis. However, Vitamin D functions within two systems in the human body:
Two of the possible effects of vitamin D are in reducing uric acid and inflammation. As ldl cholesterol is a marker for inflammation my experience is that supplementation with vitamin D has shown up markedly in my lipid and uric acid levels in the following graph. I had been gradually increasing my uric acid, triglyceride and ldl-c levels (consistent with insulin resistance) up until I adopted a lifestyle intervention around the beginning of 2014. My supplementation of vitamin D began around October/November 2015. 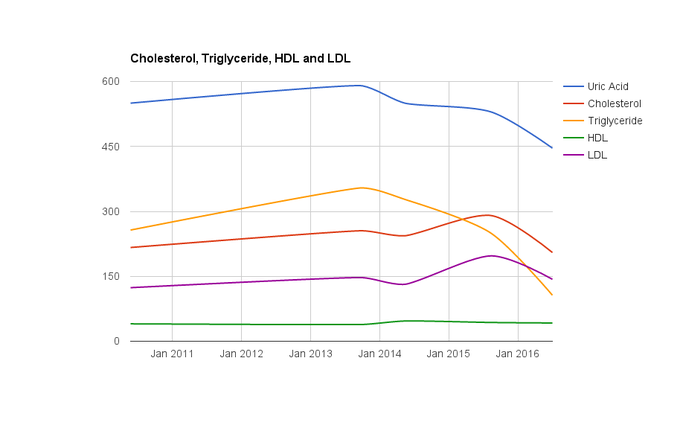 Lipids are shown in US units (mg/dl) while uric acid is in SI units to make them fit on a graph conveniently I am aware that in some people vitamin D at high doses can lead to hypercalcaemia, my understanding is that ensuring adequate levels of K2 will ensure that the calcium will be deposited in bone (where it is wanted) and not in soft tissue such as arteries. While I suspect that I already have good intake of K2 through food sources I also supplement at 100 mcg daily as an added precaution.
I am 63 and on no medications apart from the D3 and K2 which I supplement. I believe that I was approaching a state of pre-diabetes until I took charge of my own health and intervened in lifestyle choices. One of those choices was to supplement at a rate of 5000IU of D3, which is not excessive by overseas practice. While I understand it is possible for me to get a prescription from my doctor to qualify for 'reasonable excuse' under your guidelines, I foresee a potential conflict in that my doctor is guided by you and will potentially be going against your concept of 'best practice' unless he follows your published criteria. As it was, he refused to schedule a lab test for 25(OH)D when I wanted one back in 2015, which refusal caused me to have to pay $40 for my own assay. From my position it seems that guidelines from authorities like Ministry of Health on the likes of 'healthy eating' and 'healthy sun exposure' as well as setting lower criteria for prescribing statin medications, are resulting in increasingly poor health outcomes for New Zealanders. I have reversed some poor trends in my own health by ignoring such guidelines and following my own research. To be forced to abide by MOH regulations for my vitamin D supplementation is putting my health at unnecessary risk and I hope you will take the content of my letter as being 'reasonable excuse' for allowing my D3 supplement through the border.
1 Comment
|
Gregg SheehanProblem solver from way back. Currently working on the challenge of weight and health. Hence this website. Archives
November 2020
Categories
All
|
Gregg's Diet Shack
- Journey
- Index
-
Basics
- Discussions by Subject >
- Foods - Nobody does it better than Georgia Ede >
-
The People
>
- Rosedale Lecture
- All Sorts of Links and Videos
- The 20 Myths
- Diet and Nutrition for the Australian People
- Diet, Nutrition and Biochemistry Blogs and Websites
- Discussion on the 'life expectancy' myth
- Micronutrients Veg vs. Meat
- Human History >
- The Fat of the Land
-
Diseases
-
The Studies
- Tools
- Blog
- Quotes
- Recipes
- Articles
- Contact
- RDA
- Liver Flush
- Smacking
- Controversy
- Whisky
- Lentils
- Chad
- IQ
- False
- Falseinfo
- factcheckgood
- factcheckivermectin
- TGC-Licence
- Moccasins
- totalgym
- Law
- Scooters
- Nami
 RSS Feed
RSS Feed
